Shoulder Impingement Explained: What Subacromial Pain Syndrome Really Is — and How Physiotherapy Helps
Shoulder impingement — now more accurately referred to as subacromial pain syndrome (SAPS) — is one of the most common causes of shoulder pain we see at AlphaCare Physio. The good news? For most people, it is very treatable with the right rehabilitation plan, without surgery.
Rather than being caused by a single injury or “bone spur,” subacromial pain syndrome usually develops due to overload, movement patterns, and strength imbalances over time.
What Is Shoulder Impingement (Subacromial Pain Syndrome)?
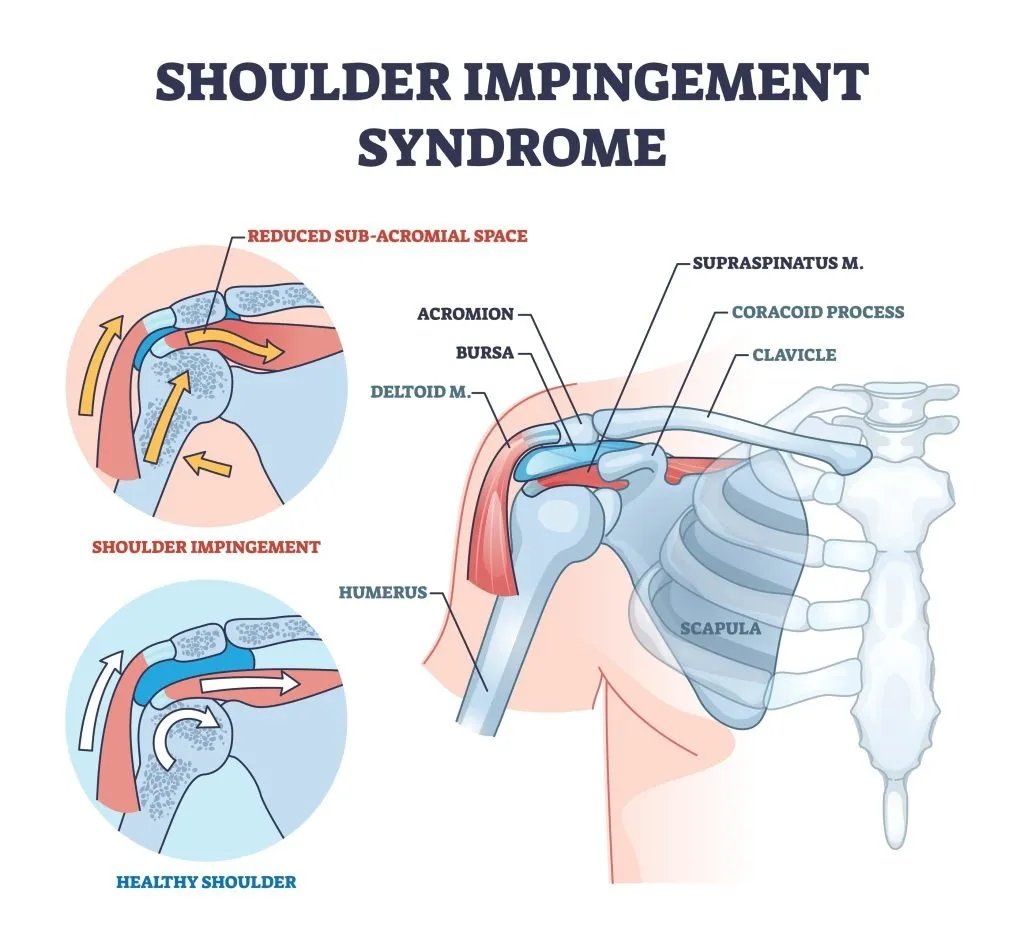
Subacromial pain syndrome refers to pain caused by irritation of the rotator cuff tendons and/or the subacromial bursa as they move through the space beneath the acromion (the bony roof of the shoulder).
Pain is typically felt:
- At the front or outer side of the shoulder
- When lifting the arm away from the body or overhead
- Most noticeably between shoulder height and overhead — known as the “painful arc”
This condition is particularly common in:
- People over 35–40 years
- Overhead workers (trades, labourers)
- Gym-goers and athletes
- Anyone performing repetitive upper-limb tasks
What Causes Shoulder Impingement?
Shoulder impingement is rarely caused by one single factor. Instead, it usually develops due to a combination of load, movement, and tissue capacity.
Common contributing factors include:
Muscle weakness or imbalance
Weakness in the rotator cuff or shoulder blade (scapular) muscles can alter how the shoulder joint moves, increasing strain on sensitive tissues.
Repetitive or overhead loading
Activities such as lifting, throwing, swimming, painting, gym pressing, or repetitive work can gradually overload the shoulder structures.
Postural and mobility factors
Rounded shoulders, forward head posture, or a stiff upper back (thoracic spine) can change shoulder mechanics and reduce load tolerance.
Age-related changes
Normal age-related changes — such as rotator cuff tendinopathy, bursal thickening, AC joint arthritis, or variations in acromial shape — can reduce space under the acromion. Importantly, many of these changes are also seen in pain-free shoulders.
👉 This is why pain is not simply explained by scan findings alone.
Common Symptoms of Shoulder Impingement
You may notice:
- Pain when lifting the arm between 70–120 degrees
- Discomfort with overhead tasks (hanging washing, reaching cupboards, gym presses)
- Pain that eases when the arm rests by your side
- Night pain, especially lying on the affected shoulder
- Stiffness after rest
- Weakness, fatigue, or a “catching” sensation
How Is Shoulder Impingement Diagnosed?
Most cases of subacromial pain syndrome are diagnosed clinically, without the need for immediate imaging.
A physiotherapist will assess:
- Shoulder posture and movement
- Range of motion
- Rotator cuff and scapular strength
- Symptom response during specific tests (e.g. painful arc, Hawkins–Kennedy)
Do I need a scan?
Ultrasound or MRI may be considered if:
- Symptoms persist despite good rehab
- There was a traumatic injury
- There is concern about a significant rotator cuff tear
Current guidelines recommend clinical assessment over imaging alone, as many scan “abnormalities” are common in people without pain.
Evidence-Based Treatment for Shoulder Impingement
✅ Physiotherapy is first-line treatment
Research strongly supports exercise-based rehabilitation as the most effective treatment for subacromial pain syndrome.
Core components of physiotherapy include:
- Individualised rotator cuff and scapular strengthening
- Gradual, phased loading rather than rest
- Pain-appropriate mobility and isometric exercises early on
- Progression to functional, work- or sport-specific strength
- Education around load management and technique
Manual therapy and soft-tissue techniques may be used as adjuncts to improve comfort and movement tolerance, especially in early stages.
💊 Medication and injections
- Short-term pain relief (e.g. paracetamol or NSAIDs) may help you participate in rehab
- Corticosteroid injections may provide temporary relief for severe or persistent pain but are most effective when combined with rehabilitation, not used alone
Is Surgery Necessary?
For most people, no.
High-quality research and Australian guidelines show that subacromial decompression surgery provides little to no benefit over good conservative care for the majority of patients.
Surgery is considered only when:
- Symptoms remain severe and function-limiting
- Several months of high-quality rehab have failed
- Imaging confirms a surgically relevant problem (e.g. a significant rotator cuff tear)
What Does Recovery Look Like?
Recovery timelines vary, but many people experience significant improvement within 6–12 weeks of structured physiotherapy.
Rehab focuses on:
- Reducing pain and restoring comfortable movement
- Building rotator cuff and shoulder blade strength
- Improving tolerance to overhead or higher-load activities
- Addressing contributing factors such as thoracic mobility or overall strength
👉 Long-term success depends on maintaining strength and gradually returning to load, not simply waiting for pain to disappear.
Book Your Shoulder Assessment at AlphaCare Physio
If you’re dealing with shoulder pain in Marion, Mitchell Park, or nearby suburbs, we’ll assess the true driver of your symptoms and build a clear step-by-step rehab plan to get you back to work, training, and daily life with confidence.